Right now, about half of all people who take medicine for an anxiety disorder don’t get much help from it. And doctors have no definitive way to predict who will, and who won’t, benefit from each anti-anxiety prescription they write.But a University of Michigan Medical School researcher and his team are working to bring more certainty to how doctors and patients choose anxiety treatments, by probing the connection between brain activity, genetics and medication.
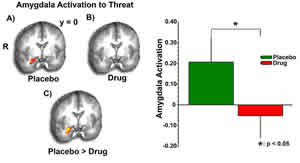
These brain scans and graph show that response to a threat was greatly reduced when study volunteers received THC, compared with placebo. This indicates that the brain’s cannabinoid system may be a good target for anxiety disorder treatments
In a paper last month in the Journal of Neuroscience, K. Luan Phan, M.D., and his former University of Chicago colleagues reported intriguing findings from a brain imaging study in occasional, non-dependent, marijuana users.
In a placebo-controlled design, they made the findings after giving the volunteers delta-9-tetrahydrocannabinol (THC), the active ingredient in marijuana, and exposing them to photographs of emotional faces, which served as signals of social communication. The study results, which showed that THC reduces the response to threat in a brain region called the amygdala, allowed the researchers to zero in on an area of the brain that might serve as a good target for new anti-anxiety drugs.
Now, with a new clinical trial that is currently seeking participants, Phan is searching for more clues as to how anxiety treatment could be tailored to the individual patient, to give the best chance that a treatment will work for him or her.
The new study will test a generic form of the drug Zoloft (sertraline), a selective serotonin reuptake inhibitor (SSRI) approved by the U.S. Food and Drug Administration for social anxiety disorder and other anxiety disorders. Both people with social anxiety disorder and a comparison group of people without anxiety are needed for brain scanning and genetic testing.
The idea is to see whether variations in the genes for certain brain receptors and transporters are linked with variations in how a person’s brain reacts to pictures of emotional faces, and variations in how they respond to the anti-anxiety drug. This information could lead to an individualized or personalized approach to medical care.
“These two studies are trying to get to the same goal: to find better treatments for anxiety disorders that affect millions of Americans and seriously interfere with their functioning,” says Phan, an assistant professor of psychiatry at U-M and the VA Ann Arbor Healthcare System. “The cannabis study highlights a new avenue that we need to explore further as we try to develop novel medications, while the sertraline study will try to find out if we can tell which patients might or might not respond well, and by what mechanism, to an already existing medication known to have some efficacy in treating anxiety disorders.”
More information about the new study is available on the U-M Engage Web site, or via 734-232-0199 or socialphobia@umich.edu.
Phan led the cannabis study at the University of Chicago, collaborating with Harriet deWit, Ph.D., the director of the Human Behavioral Pharmacology Laboratory in the Department of Psychiatry there. Their results are based on brain scans of 16 recreational marijuana users who agreed to undergo functional magnetic resonance imaging, or fMRI.
The researchers chose fMRI because it allows them to see in real time which areas of the brain are most active while a volunteer is performing a certain task – for example, viewing a picture of a human face that is expressing anger or fear, or performing a decision-making exercise.
That same approach will be used in the new sertraline study, with two different scans before and after anxiety patients are prescribed the medication. The healthy volunteers in the study will also have fMRI scans, though they will not receive the drug. All study participants must between 18 and 55 years old, and those with anxiety disorders must not be taking any other medication that could be affecting the brain in order to qualify to enter the study.
The cannabis study used THC, and a placebo caplet that looked exactly like the THC caplet. The researchers found that when the marijuana users received THC, their brain’s response to “threatening” faces was less than it was when they received a placebo.
The difference in response was seen in an area of the brain called the amygdala, which is a hub for the brain’s ability to process signs of danger or warning, and to decide how to respond. But there were no differences between THC and placebo in the areas of the brain that process non-emotional visual signals or govern body movement – suggesting that THC had a specific effect on a specific brain region and on a specific task of processing fear. Other researchers have shown this to be a region that’s rich in a receptor called CB1, part of the brain’s “cannabinoid” system.
The human brain produces compounds called endocannabinoids that act on these receptors, and are involved in anxiety and fear-learning, or the learning of which threats to be afraid of. But little has been known about the effect of THC, an exogenous cannabinoid, on the brain’s own system.
For ethical reasons, the researchers did not give THC to non-marijuana users, and the study was small. But the findings in the study volunteers suggest that THC and other compounds that act on the CB1 receptors in the amygdala could be fruitful targets for new anti-anxiety medicines. Phan notes that rimonabant, a smoking-cessation and weight-loss drug not yet available in the United States for clinical use, also acts on the CB1 receptor.
Understanding how drugs such as marijuana affect the brain may also help reveal more about why people become addicted to illicit drugs or abuse certain prescription drugs, Phan notes. Some individuals may be using illicit drugs and misusing prescribed drugs to alleviate their anxiety. He hopes to investigate this issue further by studying people who have used prescription pain drugs recreationally (such as oxycodone), using new funding from the National Institutes of Health.
The THC study links three key domains of human behavior: a specific region of the brain, the function of that area, and a neurochemical agent (THC) that appears to act on them. The new sertraline study will take it one step further, by looking at genetics too. Specifically, Phan and his colleagues will look for variations (“functional polymorphisms”) among several genes in individual subjects. Key among them is the gene (5-HTTLPR) that encodes the serotonin transporter protein that transports the neurotransmitter serotonin in and out of brain cells. Serotonin has long been known to be involved in depression and anxiety, and indeed most modern antidepressant and anti-anxiety drugs (such as SSRIs) work on this transporter.
Reference: Journal of Neuroscience, March 5, 2008, Vol. 28, No. 10, 2313-2319
Written by: Kara Gavin
Source : University of Michigan